
In Chennai more than 50% deliveries are Caesarian..Is the safety of Mom the prime criterion for ruling out natural delivery? I guess the pecuniary considerations outweigh safety...I did not know this is a global phenomenon until I read this!
[h=3]Caesar’s legions[/h] [h=1]The global rise of Caesarean sections is being driven not by medical necessity but by growing wealth—and perverse financial incentives for doctors[/h] Aug 15th 2015 | NEW YORK AND SÃO PAULO | From the print edition
A YEAR ago a hospital in São Paulo announced that its maternity ward would henceforth only admit clients from 10am to 4pm, Monday to Friday. The message was clear: births by appointment only—that is, by Caesarean section. For Arthur Chioro, Brazil’s health minister, it was equally unequivocal: the country’s attitude to birth “has become absurd”.
In 2009 Brazil became the first country where less than half of babies were born as nature intended. At the last count, in 2013, fully 57% of births were by Caesarean section, in which the baby is delivered through an incision in the abdomen and uterus—almost double the proportion two decades ago. In Brazil’s private health-care system, Caesareans now account for nearly nine in ten births. Brazilian mothers say, only half jokingly, that their obstetricians would not know how to pull out a baby without cutting them open.
A recent study of 21 countries published in the Lancet, a medical journal, estimated that 31% of births were by Caesarean section in 2010-11. The rate is rising almost everywhere. The Dominican Republic and Egypt have joined Brazil in the greater-than-half club.
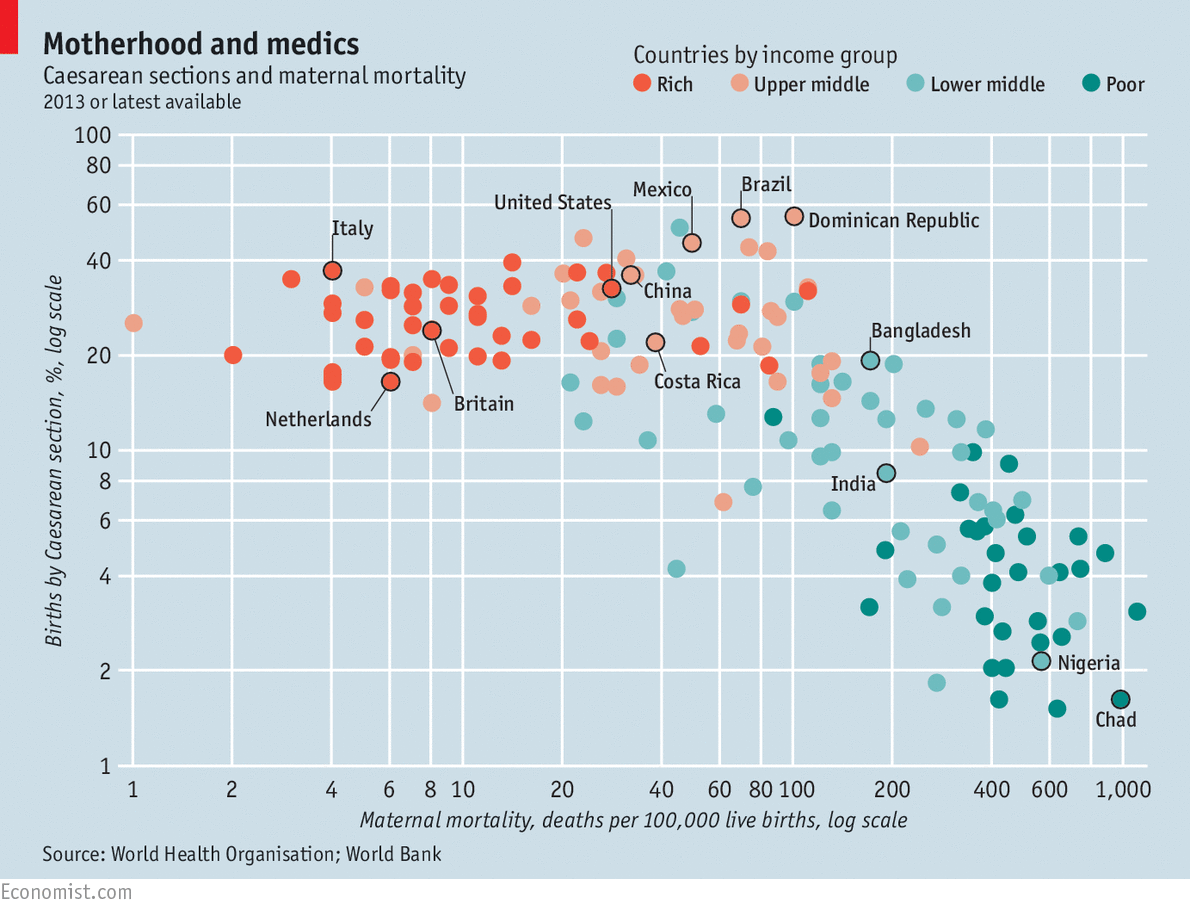
In many poor countries, C-sections are dangerously rare. In Chad, for example, less than 2% of babies are thought to be delivered this way. In other words, many Chadian women who need a C-section cannot get one—and many die as a result, as do many Chadian babies. Globally, more surgery is associated with fewer maternal deaths—but only until the proportion of babies delivered by C-section reaches about 10-15%. Above that level, more surgery does not mean fewer deaths in childbirth. Nor are babies saved.
As with any major surgery, C-sections sometimes cause complications such as haemorrhage and infection. A large Canadian study found that otherwise healthy women whose babies were breech (head-up rather than head-down) and who opted for a C-section before they went into labour were three times more likely to experience emergencies such as shock or cardiac arrest than those who delivered their babies vaginally. The procedure also increases the chance of problems in future pregnancies, such as placenta previa, when the placenta blocks the baby’s exit through the cervix.
Women who undergo Caesareans take longer to recover and are more likely to feel depressed after the birth. Children born by Caesarean section may suffer, too, as a result of not picking up bacteria in the birth canal. A study from the University of Copenhagen found that of the 2m children born in Denmark between 1977 and 2012, the 14% who had been born by Caesarean section were much more likely to suffer from ailments including asthma, juvenile arthritis and bowel inflammation.
So why has the procedure become so common? One explanation is that people are wealthier and more able to pay for surgery. Another is that expectant mothers are often older and heavier than in the past, making birth more complicated. A study of low-risk, first-time expectant mothers in Norway found that those aged over 40 were three times as likely to have their babies delivered by emergency Caesarean than women in their early 20s.
But otherwise similar countries often have quite different C-section rates. Mexico is about as wealthy as Costa Rica, but the two countries have rates of 46% and 22%. The procedure is more than twice as common in Italy as in the Netherlands. Huge differences exist between hospitals and individual obstetricians even in a single country. American hospitals’ rates vary from 7% to 70%.
In Brazil, C-sections were for years offered together with sterilisation; the combination was not banned until 1996. And for a long time natural birth was traumatic, says Regina Torloni, a former obstetrician. The state health service, known as SUS, only started paying for pain-blocking epidurals in 1998. As incomes and enrolment in private health plans have shot up in the past decade, more Brazilian women have decided they are too posh to push. The fear of getting stuck in one of São Paulo’s epic traffic jams while in labour probably makes some keener on a birth that can be scheduled in advance.
Still, a study last year found that at the start of pregnancy, two-thirds of Brazilian women wished to deliver vaginally. That less than half end up doing so suggests they are being steered.
Hospitals’ neonatal wards profit handsomely from Caesareans, which tend to be performed pre-term. So do obstetricians, who are generally paid per delivery. In the time it takes to assist a single natural birth, a medic might perform several Caesareans. Some charge patients who insist on the time-consuming natural route “standby fees”, though they are not supposed to. Many doctors are wary of malpractice suits involving complications from natural births. Obstetricians are hit with even more lawsuits than plastic surgeons.
All this has combined to “medicalise birth”, laments Ana Cristina de Andrade, an activist. Midwives like her, common in rich-world maternity wards, are scarce in Brazil. The country trains just 60 a year, at one college in São Paulo, and only since 2005. Health plans make no provision to pay them (or the more numerous specialist nurses); only doctors.
Some of these pressures are felt in rich countries, too. Economists at the University of Toronto analysed data from nearly 5m hospital records between 1994 and 2010 in Canada, where the Caesarean rate is now 27%. When doctors earned twice as much for a C-section as for a vaginal delivery, they were 6% more likely to choose it than when the two procedures paid the same. American doctors can grow impatient if labour is not progressing swiftly enough, particularly at the end of a shift or before a weekend. An analysis of three years of American data by Consumer Reports, a non-profit magazine, found that far fewer babies were born on public holidays.
 INTERACTIVE: Clic/tap here for an interactive version of this chart
INTERACTIVE: Clic/tap here for an interactive version of this chart
Fear of lawsuits is widespread, says Ana Pilar Betrán of the World Health Organisation. Aggrieved patients are more likely to sue over heroic measures not taken than for needless but standard interventions. One study estimated that nearly three-quarters of all American obstetrician-gynaecologists would face a malpractice claim by the time they were 45. They were the most likely of all specialists to have to make payouts exceeding $1m.
Jim Zhang of Shanghai Jiao Tong University says that Chinese parents, anxious about creating a perfect baby that might be their only one, can demand compensation from obstetricians who are thought to have erred. Some protest outside hospitals until they have been paid off. The association of certain dates and numbers with good fortune also means Chinese women are keen to give birth on an auspicious day. Many also fear pain—hospitals often provide little pain relief—and believe that a baby born with a perfectly round head, rather than the distortion common after a vaginal delivery, is better off.
Untimely ripped
In Egypt some women ask for a C-section because they believe it is the safest way to give birth, says Hany Abdel-Aleem, an obstetrician in Assiut. Latin Americans often believe that women who have had one can start to have sex again sooner than those who give birth vaginally, says Dr Betrán of the WHO. Still, most patients get their cues from doctors. A study of women in Shanghai, where the Caesarean rate is 57%, found that most were influenced by their health-care providers.
A few countries are now trying to reverse the trend. In Britain, where more than a quarter of deliveries are via Caesarean, twice as high a share as in 1990, the National Health Service provides expectant mothers with information about the risks, and maternity services with information about how to avoid unnecessary procedures. China’s government has begun to warn of the complications women may run into if they want another child after a C-section.
Individual hospitals have done more. Hoag Memorial Hospital Presbyterian in California, which delivers 6,000 babies a year, cut its C-section rate from 38% of births to 33% in just three years after a big health insurer threatened to exclude it because of its high maternity costs. It shared information with its staff about Caesarean rates for individual doctors, made it harder to schedule a surgical delivery, informed patients about the risks and paid bonuses to particularly helpful nurses. It also agreed to charge the same for Caesareans as for normal deliveries.
Even in Brazil, a few birth clinics staffed solely by midwives and nurses are cropping up. With budgets tight, the health ministry is keen to trim unnecessary spending on surgery. If the Caesarean rate in state SUS hospitals had been 30% instead of 40% in 2010-14, the government would have saved 772m reais ($220m), it reckons—enough to add 2,000 neonatal cots a year.
Some private hospitals are trying to spare the scalpel, too. Last December the Albert Einstein hospital in São Paulo, Brazil’s swankiest, teamed up with the Institute for Healthcare Improvement, a research outfit, and the National Supplementary Health Agency, which regulates the sector, in a pilot project to help 28 hospitals brush up on natural-birth techniques. They want to tweak incentives for doctors and midwives so that Caesareans become less appealing. Last month the agency decreed that hospitals’ and individual physicians’ Caesarean rates must be given to patients who request them.
At 68%, the Einstein’s rate remains too high, concedes Rita Sanchez, an obstetrician at the hospital who co-ordinates the project. But three floors above the sterile Caesarean ward, state-of-the-art natural-delivery rooms—complete with a jacuzzi (for natural pain relief), a big rubber ball (to loosen the hips) and surgical lamps mounted inconspicuously in the ceiling (to avoid that operating-theatre vibe)—are increasingly sought-after, Dr Sanchez reports.
Many hospitals lack such facilities, or indeed any non-surgical ones. Demand for them is rising, but only slowly. More role models like Kate Middleton in Britain, who recently gave birth naturally to a second royal baby, are needed, says Amanda Meskauskas, the administrator of Casa Angela, a charity-run birth clinic. “A telenovela would be great,” sighs Dr Sanchez, referring to Brazil’s popular soap operas, which have often championed social causes.
On a recent Sunday 15-odd expectant mothers, with flummoxed fathers-to-be in tow, shared tales of doctor discouragement. One woman was asked to pick a birth date when just eight weeks pregnant; another was told that natural birth is for cave-women. These women are motivated to avoid C-sections. Still, Ms Meskauskas estimates that more than a third will end up having one.
http://www.economist.com/news/inter...ecessity?fsrc=scn/tw/te/pe/ed/CasesarsLegions
[h=3]Caesar’s legions[/h] [h=1]The global rise of Caesarean sections is being driven not by medical necessity but by growing wealth—and perverse financial incentives for doctors[/h] Aug 15th 2015 | NEW YORK AND SÃO PAULO | From the print edition
A YEAR ago a hospital in São Paulo announced that its maternity ward would henceforth only admit clients from 10am to 4pm, Monday to Friday. The message was clear: births by appointment only—that is, by Caesarean section. For Arthur Chioro, Brazil’s health minister, it was equally unequivocal: the country’s attitude to birth “has become absurd”.
In 2009 Brazil became the first country where less than half of babies were born as nature intended. At the last count, in 2013, fully 57% of births were by Caesarean section, in which the baby is delivered through an incision in the abdomen and uterus—almost double the proportion two decades ago. In Brazil’s private health-care system, Caesareans now account for nearly nine in ten births. Brazilian mothers say, only half jokingly, that their obstetricians would not know how to pull out a baby without cutting them open.
A recent study of 21 countries published in the Lancet, a medical journal, estimated that 31% of births were by Caesarean section in 2010-11. The rate is rising almost everywhere. The Dominican Republic and Egypt have joined Brazil in the greater-than-half club.
In many poor countries, C-sections are dangerously rare. In Chad, for example, less than 2% of babies are thought to be delivered this way. In other words, many Chadian women who need a C-section cannot get one—and many die as a result, as do many Chadian babies. Globally, more surgery is associated with fewer maternal deaths—but only until the proportion of babies delivered by C-section reaches about 10-15%. Above that level, more surgery does not mean fewer deaths in childbirth. Nor are babies saved.
As with any major surgery, C-sections sometimes cause complications such as haemorrhage and infection. A large Canadian study found that otherwise healthy women whose babies were breech (head-up rather than head-down) and who opted for a C-section before they went into labour were three times more likely to experience emergencies such as shock or cardiac arrest than those who delivered their babies vaginally. The procedure also increases the chance of problems in future pregnancies, such as placenta previa, when the placenta blocks the baby’s exit through the cervix.
Women who undergo Caesareans take longer to recover and are more likely to feel depressed after the birth. Children born by Caesarean section may suffer, too, as a result of not picking up bacteria in the birth canal. A study from the University of Copenhagen found that of the 2m children born in Denmark between 1977 and 2012, the 14% who had been born by Caesarean section were much more likely to suffer from ailments including asthma, juvenile arthritis and bowel inflammation.
So why has the procedure become so common? One explanation is that people are wealthier and more able to pay for surgery. Another is that expectant mothers are often older and heavier than in the past, making birth more complicated. A study of low-risk, first-time expectant mothers in Norway found that those aged over 40 were three times as likely to have their babies delivered by emergency Caesarean than women in their early 20s.
But otherwise similar countries often have quite different C-section rates. Mexico is about as wealthy as Costa Rica, but the two countries have rates of 46% and 22%. The procedure is more than twice as common in Italy as in the Netherlands. Huge differences exist between hospitals and individual obstetricians even in a single country. American hospitals’ rates vary from 7% to 70%.
In Brazil, C-sections were for years offered together with sterilisation; the combination was not banned until 1996. And for a long time natural birth was traumatic, says Regina Torloni, a former obstetrician. The state health service, known as SUS, only started paying for pain-blocking epidurals in 1998. As incomes and enrolment in private health plans have shot up in the past decade, more Brazilian women have decided they are too posh to push. The fear of getting stuck in one of São Paulo’s epic traffic jams while in labour probably makes some keener on a birth that can be scheduled in advance.
Still, a study last year found that at the start of pregnancy, two-thirds of Brazilian women wished to deliver vaginally. That less than half end up doing so suggests they are being steered.
Hospitals’ neonatal wards profit handsomely from Caesareans, which tend to be performed pre-term. So do obstetricians, who are generally paid per delivery. In the time it takes to assist a single natural birth, a medic might perform several Caesareans. Some charge patients who insist on the time-consuming natural route “standby fees”, though they are not supposed to. Many doctors are wary of malpractice suits involving complications from natural births. Obstetricians are hit with even more lawsuits than plastic surgeons.
All this has combined to “medicalise birth”, laments Ana Cristina de Andrade, an activist. Midwives like her, common in rich-world maternity wards, are scarce in Brazil. The country trains just 60 a year, at one college in São Paulo, and only since 2005. Health plans make no provision to pay them (or the more numerous specialist nurses); only doctors.
Some of these pressures are felt in rich countries, too. Economists at the University of Toronto analysed data from nearly 5m hospital records between 1994 and 2010 in Canada, where the Caesarean rate is now 27%. When doctors earned twice as much for a C-section as for a vaginal delivery, they were 6% more likely to choose it than when the two procedures paid the same. American doctors can grow impatient if labour is not progressing swiftly enough, particularly at the end of a shift or before a weekend. An analysis of three years of American data by Consumer Reports, a non-profit magazine, found that far fewer babies were born on public holidays.
INTERACTIVE: Clic/tap here for an interactive version of this chart Fear of lawsuits is widespread, says Ana Pilar Betrán of the World Health Organisation. Aggrieved patients are more likely to sue over heroic measures not taken than for needless but standard interventions. One study estimated that nearly three-quarters of all American obstetrician-gynaecologists would face a malpractice claim by the time they were 45. They were the most likely of all specialists to have to make payouts exceeding $1m.
Jim Zhang of Shanghai Jiao Tong University says that Chinese parents, anxious about creating a perfect baby that might be their only one, can demand compensation from obstetricians who are thought to have erred. Some protest outside hospitals until they have been paid off. The association of certain dates and numbers with good fortune also means Chinese women are keen to give birth on an auspicious day. Many also fear pain—hospitals often provide little pain relief—and believe that a baby born with a perfectly round head, rather than the distortion common after a vaginal delivery, is better off.
Untimely ripped
In Egypt some women ask for a C-section because they believe it is the safest way to give birth, says Hany Abdel-Aleem, an obstetrician in Assiut. Latin Americans often believe that women who have had one can start to have sex again sooner than those who give birth vaginally, says Dr Betrán of the WHO. Still, most patients get their cues from doctors. A study of women in Shanghai, where the Caesarean rate is 57%, found that most were influenced by their health-care providers.
A few countries are now trying to reverse the trend. In Britain, where more than a quarter of deliveries are via Caesarean, twice as high a share as in 1990, the National Health Service provides expectant mothers with information about the risks, and maternity services with information about how to avoid unnecessary procedures. China’s government has begun to warn of the complications women may run into if they want another child after a C-section.
Individual hospitals have done more. Hoag Memorial Hospital Presbyterian in California, which delivers 6,000 babies a year, cut its C-section rate from 38% of births to 33% in just three years after a big health insurer threatened to exclude it because of its high maternity costs. It shared information with its staff about Caesarean rates for individual doctors, made it harder to schedule a surgical delivery, informed patients about the risks and paid bonuses to particularly helpful nurses. It also agreed to charge the same for Caesareans as for normal deliveries.
Even in Brazil, a few birth clinics staffed solely by midwives and nurses are cropping up. With budgets tight, the health ministry is keen to trim unnecessary spending on surgery. If the Caesarean rate in state SUS hospitals had been 30% instead of 40% in 2010-14, the government would have saved 772m reais ($220m), it reckons—enough to add 2,000 neonatal cots a year.
Some private hospitals are trying to spare the scalpel, too. Last December the Albert Einstein hospital in São Paulo, Brazil’s swankiest, teamed up with the Institute for Healthcare Improvement, a research outfit, and the National Supplementary Health Agency, which regulates the sector, in a pilot project to help 28 hospitals brush up on natural-birth techniques. They want to tweak incentives for doctors and midwives so that Caesareans become less appealing. Last month the agency decreed that hospitals’ and individual physicians’ Caesarean rates must be given to patients who request them.
At 68%, the Einstein’s rate remains too high, concedes Rita Sanchez, an obstetrician at the hospital who co-ordinates the project. But three floors above the sterile Caesarean ward, state-of-the-art natural-delivery rooms—complete with a jacuzzi (for natural pain relief), a big rubber ball (to loosen the hips) and surgical lamps mounted inconspicuously in the ceiling (to avoid that operating-theatre vibe)—are increasingly sought-after, Dr Sanchez reports.
Many hospitals lack such facilities, or indeed any non-surgical ones. Demand for them is rising, but only slowly. More role models like Kate Middleton in Britain, who recently gave birth naturally to a second royal baby, are needed, says Amanda Meskauskas, the administrator of Casa Angela, a charity-run birth clinic. “A telenovela would be great,” sighs Dr Sanchez, referring to Brazil’s popular soap operas, which have often championed social causes.
On a recent Sunday 15-odd expectant mothers, with flummoxed fathers-to-be in tow, shared tales of doctor discouragement. One woman was asked to pick a birth date when just eight weeks pregnant; another was told that natural birth is for cave-women. These women are motivated to avoid C-sections. Still, Ms Meskauskas estimates that more than a third will end up having one.
http://www.economist.com/news/inter...ecessity?fsrc=scn/tw/te/pe/ed/CasesarsLegions